Chong Hua Hospital Patient Portal
Chong Hua Hospital Patient Portal
Patient Registration Form
Please fill in all the required fields. Fields marked in asterisk (
*
) are mandatory
With Patient No.
Without Patient No.
User Account
Patient No.
*
Password
*
Confirm Password
*
Contact Information
Email
*
Mobile No. (11-Digit)
*
Personal Information
First Name
*
Middle Name
*
Last Name
*
Suffix
-
JR.
SR.
II
III
IV
V
VI
VII
VIII
IX
Birthday
*
Month
January
February
March
April
May
June
July
August
September
October
November
December
Day
Year
Gender
*
-
MALE
FEMALE
×
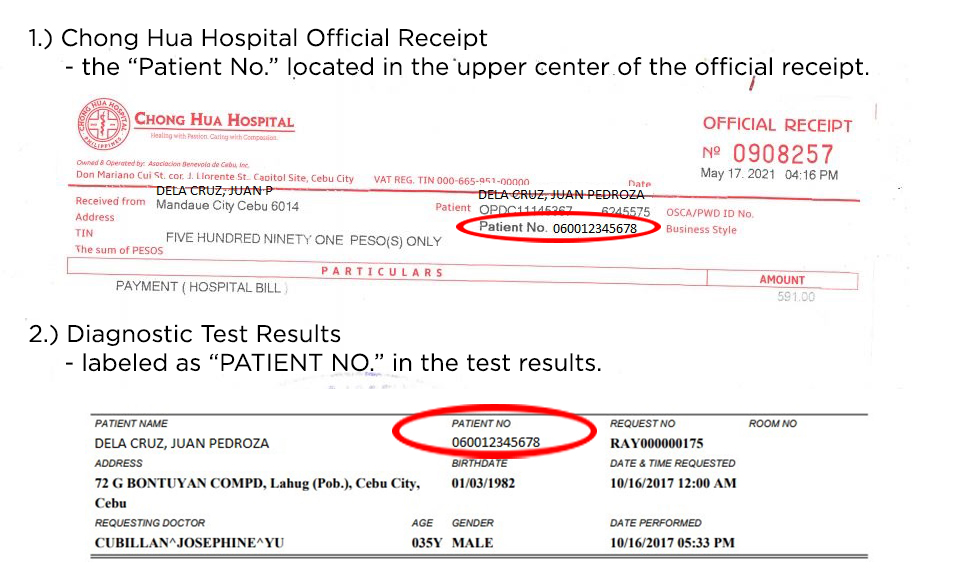
Patient No. is located in